
Hair Loss
Understanding your hair loss
Everyone loses some hair every day. Losing up to 100 hairs a day is normal.
Call 650-638-1226 or click here to email us or here for a free eBook on hair restoration options.
But if hair loss runs in your family, you could lose a lot more hair. With this kind of hair loss, you may end up with bald spots if you are a man. If you are a woman, you may find that the hair on the top of your head is slowly thinning. About half of all people have this type of hair loss by around age 50.
Although hair loss is fairly common, it can be a tough thing to live with, especially when it changes how you look. But there are ways you can treat your hair loss.
 First step to treating hair loss is the correct diagnosis
First step to treating hair loss is the correct diagnosis
 First step to treating hair loss is the correct diagnosis
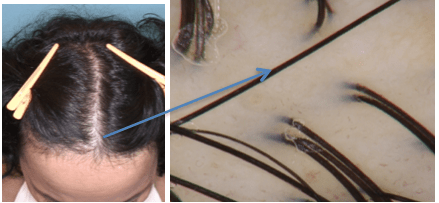
First step to treating hair loss is the correct diagnosisThe first step towards finding the right treatment for your hair loss is determining the correct diagnosis. At the Silicon Valley Hair Institute, we have advanced High Defintion Hair Dermoscopy to assist Dr. Canales in diagnosing, treating and monitoring your hair loss treatment progress.
Causes of hair loss can include:
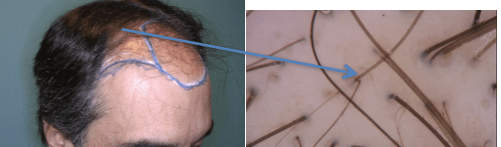
- Androgenetic alopecia in men (MPHL) Androgenetic alopecia (AGA) is a condition related to the influence of androgen hormones on hair follicles. Androgens may stimulate a slow transformation and finally the “deactivation” of the hair follicle (the so-called miniaturization). It is observed in people with genetic predispositions and often runs in the family. In the Caucasian population, androgenetic alopecia is observed in 80% of men and approximately 40% of women. In people of Asian descent and African Americans, the prevalence of AGA is lower.
Symptoms: The first symptoms of androgenetic alopecia may appear in one’s teens. Sometimes, the recession of the hairline in the temporal and frontal areas dominates, whereas in other persons, the thinning of hair in the vertex area may dominate. Most often, the density and thickness of hair in the occipital area remains nearly unchanged, which results from a much lesser sensitivity of these hair follicles to hormonal stimuli. Patients often note a slow gradual replacement of thick, typically colored hair with thinner and softer hair. Some hair is gradually transformed into clinically invisible, very short , nearly transparent hair. In men, the androgenetic alopecia process may cover the whole scalp area.
, nearly transparent hair. In men, the androgenetic alopecia process may cover the whole scalp area.
Course of disease: The condition is progressive. The first symptoms of the androgenetic alopecia may appear before age 20. Male androgenetic alopecia may lead to complete hair loss.
Diagnosis: The diagnosis is made based on the clinical picture. Trichoscopy is used to confirm the diagnosis and rule out other conditions connected with hair loss.
Treatment: Surgical restoration of balding areas may be achieved with robotic hair transplantation (robotic FUE), and/or Follicular Unit Transplantation (FUT). Medical treatment is most efficient with the early application of therapy (hair follicles miniaturization is reversible only to a certain extent). In treatment, 5-α-reductase inhibitors, finasteride and dutasteride are used. Preparations of minoxidil and prostaglandin analogs are used topically. Other treatments may be effective; consult your doctor to explore other options. - Androgenetic alopecia in women (FPHL) Androgenetic alopecia (AGA) is a condition related to the influence of androgen hormones on hair follicles. Androgens may stimulate a slow transformation and finally the “deactivation” of the hair follicle (so-called miniaturization). It is observed in people with genetic predispositions and often runs in the family. In the Caucasian population, androgenetic alopecia is observed in 80% of men and approximately 40% of women. In people of Asian descent and African Americans, the prevalence of AGA is lower. Androgenetic alopecia in women is often called by the abbreviation FAGA (female androgenetic alopecia) or FPHL (female pattern hair loss).
Symptoms: Female androgenetic alopecia may have different clinical presentations. Often, it is related to hair thinning, with the so-called Christmas tree sign, where the thinning of hair is more visible near the forehead and less visible towards the vertex. Less frequently, diffuse hair thinning is accompanied by the recession of the hairline in temporal areas. All these conditions give a clinical picture of marked variation of hair thickness between the frontal and occipital areas. Moreover, the number of hair units with more than one hair decreases; they are replaced by single-hair units. Androgenetic alopecia may be a symptom of hormonal disorders, such as polycystic ovaries syndrome (PCO), and may accompany such conditions as insulin resistance or metabolic syndrome. Androgenetic alopecia may be accompanied by seborrhea.
Course of disease: The condition is progressive. First symptoms of the androgenetic alopecia may appear before age 20. In females, complete hair loss does not occur.
Diagnosis: Beside clinical examination, trichoscopy plays an important role in diagnosing AGA. Trichoscopy allows to differentiate the condition from other types of hair loss. It is particularly important due to the fact that androgenetic alopecia may be accompanied by chronic telogen effluvium. Sometimes, laboratory tests are recommended to rule out the possibility of coexistence of hormonal disorders.
Trichoscopy allows to differentiate the condition from other types of hair loss. It is particularly important due to the fact that androgenetic alopecia may be accompanied by chronic telogen effluvium. Sometimes, laboratory tests are recommended to rule out the possibility of coexistence of hormonal disorders.
Treatment: The treatment of androgenetic alopecia is the more efficient the faster it is implemented as the miniaturization of hair follicles is only partially reversible. In treatment, preparations of minoxidil and 5-α-reductase inhibitors, finasteride and dutasteride are used. In women, general treatment with androgen suppressants or antagonists, such as spironolactone or cyproterone acetate and estrogen, may be introduced. Other medical options exist. Hair transplantation also has an important role in select female patients with androgenetic alopecia.
 , nearly transparent hair. In men, the androgenetic alopecia process may cover the whole scalp area.
, nearly transparent hair. In men, the androgenetic alopecia process may cover the whole scalp area.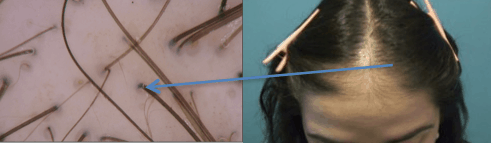 Trichoscopy allows to differentiate the condition from other types of hair loss. It is particularly important due to the fact that androgenetic alopecia may be accompanied by chronic telogen effluvium. Sometimes, laboratory tests are recommended to rule out the possibility of coexistence of hormonal disorders.
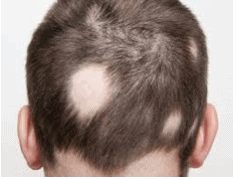
Trichoscopy allows to differentiate the condition from other types of hair loss. It is particularly important due to the fact that androgenetic alopecia may be accompanied by chronic telogen effluvium. Sometimes, laboratory tests are recommended to rule out the possibility of coexistence of hormonal disorders.- Alopecia areata: Alopecia areata (AA) is manifested by non-scarring, patchy, focal hair loss and is classified as an autoimmune disease. The prevalence of this disease in the general population is 1-2%. In 50% of patients, the disease starts in adolescen
 ce. A typical symptom is a presence of well-delimited hairless areas. The pathological mechanism leading to alopecia areata is not completely understood. The influence of genetic factors and environmental factors (including stress) is often emphasized as a trigger of the autoimmune process.
ce. A typical symptom is a presence of well-delimited hairless areas. The pathological mechanism leading to alopecia areata is not completely understood. The influence of genetic factors and environmental factors (including stress) is often emphasized as a trigger of the autoimmune process.
Symptoms: In patients, a sudden appearance of a round or oval denuded patch is observed. The number and size of patches may differ; sometimes it is one patch 1-2 cm in diameter, less frequent there are numerous, often merging bald patches. There are several forms of alopecia areata: focal alopecia, diffuse alopecia areata, ophiasis (balding in the occipital and temporal areas), alopecia totalis (hair loss of the scalp), and alopecia universalis (total body hair loss).
Course of disease: The course of the disease is hard to predict. Worse prognoses are observed in patients with an early onset of the disease, with a family history of alopecia areata, accompanying atopy, and in case of coexistence of other autoimmune diseases or nail lesions. It seems that the most important prognostic factor is the extent of the hair loss. In some patients, spontaneous remissions are observed, while in approximately 5% of patients, a progression towards total alopecia totalis is noticed, and in 1%, progression towards alopecia universalis detected. Sometimes, recurrent course of the disease is observed.
Diagnosis: The diagnosis is determined based on the clinical picture and trichoscopy. Punch biopsy maybe necessary.
Treatment: Topical administration drugs and general administration drugs are used. Immunosuppresive drugs (corticosteroids, cyclosporin), photochemotherapy (PUVA), and immunomodulation drugs are used. Other medical options exist; consult your doctor to learn more. - Frontal fibrosing alopecia (FFA)Frontal fibrosing alopecia (FFA) is a condition described by Steven Kossard in 1994. The prevalence of this condition is difficult to assess. Many authors consider FFA to be a subtype of LPP (lichen planopilaris). Scarring is a result of the lymphocytic inflammation, which leads to the permanent damage of hair follicles.
Symptoms: This condition most often affects post-menopausal women. In patients with the FFA, the percentage of pre-menopausal women does not exceed approximately 8%, while the percentage of men amounts to 2%. The main symptom is a slow gradual recession of the frontal and temporal hairlines. Rarely may the same process be observed in the parietal area. A frequent accompanying symptom is the thinning of eyebrows (especially the lateral parts) and hair in other body areas (arm pits, groins and, less frequently, limbs). Sometimes, isolated hair dispersed on previously-hairy skin may be observed. Within the newly formed hairline, no vellus hair is observed, and sometimes skin erythema is visible. In a subset of FFA patients, small reddish papules may form on the face, sometimes considered to be rough skin.
pits, groins and, less frequently, limbs). Sometimes, isolated hair dispersed on previously-hairy skin may be observed. Within the newly formed hairline, no vellus hair is observed, and sometimes skin erythema is visible. In a subset of FFA patients, small reddish papules may form on the face, sometimes considered to be rough skin.
Course of disease: The beginning of the condition is often difficult to note by a patient, and only a significant recession of the hairline is a reason to seek dermatological advice. The condition is slowly progressive; the rate of hairline recession varies from 0.3 to 1.7 mm per month. The thinning of hair within the eyebrows starts from the sides and progresses towards the middle, often leading to complete loss of eyebrows. Frontal fibrosing alopecia is irreversible.
Diagnosis: The diagnosis is determined based on the clinical picture and trichoscopy. Punch biopsy maybe necessary.
Treatment: The treatment is challenging. Steriods, retinoids, and minoxidil are often used to obtain stabilization of the pathological condition. Some authors stress the effectiveness of hydroxichloroquine, cyclosporin and mycophenolate mofetil. Other medical options exist; consult your doctor to learn more. - Lichen planopilaris (LPP) Lichen planopilaris (LPP), in its classic form, is the most frequent cause of primary alopecia in adults. LPP affects women twice as often as men. The disease proceeds with irreversible hair loss as a result of hair follicles damage by an autoimmune process.
Symptoms: Typically, at the beginning, the presence of reddish or violaceous papules or erythematous areas may be o bserved, which is accompanied by scalp scaling. The lesions often occur in the parietal and vertex area. A frequent accompanying symptom is itching and tenderness of the affected scalp. These conditions are sometimes worsened by sweating, exposure to sun, irritation and stress. When inflammatory symptoms subside, focal or diffuse alopecia may be observed, which gives an image of confluent white dots or milky-red areas.
bserved, which is accompanied by scalp scaling. The lesions often occur in the parietal and vertex area. A frequent accompanying symptom is itching and tenderness of the affected scalp. These conditions are sometimes worsened by sweating, exposure to sun, irritation and stress. When inflammatory symptoms subside, focal or diffuse alopecia may be observed, which gives an image of confluent white dots or milky-red areas.
Course of disease: The disease is often progressive, although its activity may vary between different people. At first, the affected small areas may tend to become confluent and affect large areas of the scalp. In places of scar formation, hair regrowth is impossible.
Diagnosis: The diagnosis is possible based on clinical picture and trichoscopy procedure. Sometimes a punch biopsy is necessary to confirm the diagnosis.
Treatment: In the early period of the LPP, the most important treatments are anti-inflammatory drugs, such as corticosteroids and retinoids. Some authors stress the effectiveness of hydroxichloroquine, cyclosporin and mycophenolate mofetil. The latest reports refer to PPAR modulators. Other medical options exist; consult your doctor to learn more. - Postpartum alopecia Postpartum alopecia is classified as telogen effluvium. This process depends on the influence of hormones on hair follicles; in particular, this
 influence is connected to the reduction of estradiol and tyroxine levels in the postpartum period. The influence of these hormones on hair follicles during pregnancy causes a decrease of the number of hairs in the telogen phase (inactive phase) by about half. Hair loss following childbirth is therefore an expression of the body returning to the situation from before pregnancy (hair “stopped” in active growth phase by pregnancy hormones starts to fall out, as well as hair that was supposed to fall out in this period). Some authors point out a certain correlation of postpartum alopecia with the prevalence of postpartum depression, which may be caused by the same hormonal factors.
influence is connected to the reduction of estradiol and tyroxine levels in the postpartum period. The influence of these hormones on hair follicles during pregnancy causes a decrease of the number of hairs in the telogen phase (inactive phase) by about half. Hair loss following childbirth is therefore an expression of the body returning to the situation from before pregnancy (hair “stopped” in active growth phase by pregnancy hormones starts to fall out, as well as hair that was supposed to fall out in this period). Some authors point out a certain correlation of postpartum alopecia with the prevalence of postpartum depression, which may be caused by the same hormonal factors.
Symptoms: Postpartum alopecia is diffuse (20-30% of hair from the final stage of pregnancy) and appears quite suddenly, from approximately the 2nd or 3rd month following childbirth. No complete hair loss is observed.
Course of disease: The spontaneous hair regrowth usually occurs within 6 to 9 months after childbirth. In breastfeeding women, the hair regrowth may take longer due to the influence of prolactin on hair follicles.
Diagnosis: It is simple to diagnose due to the childbirth history. A trichoscopy allows to exclude other disease entities.
Treatment: In general, no routine treatment of postpartum alopecia is used, in particular in breastfeeding women. In case of significant hormonal disorders, thyroid hormones and estradiol supplementation is implemented, and sometimes hormonal contraceptive drugs are administered. In breastfeeding women, therapeutic possibilities are limited due to the potential adverse effect on the baby. Other medical options exist; consult your doctor to learn more.
 ce. A typical symptom is a presence of well-delimited hairless areas. The pathological mechanism leading to alopecia areata is not completely understood. The influence of genetic factors and environmental factors (including stress) is often emphasized as a trigger of the autoimmune process.
ce. A typical symptom is a presence of well-delimited hairless areas. The pathological mechanism leading to alopecia areata is not completely understood. The influence of genetic factors and environmental factors (including stress) is often emphasized as a trigger of the autoimmune process. pits, groins and, less frequently, limbs). Sometimes, isolated hair dispersed on previously-hairy skin may be observed. Within the newly formed hairline, no vellus hair is observed, and sometimes skin erythema is visible. In a subset of FFA patients, small reddish papules may form on the face, sometimes considered to be rough skin.
pits, groins and, less frequently, limbs). Sometimes, isolated hair dispersed on previously-hairy skin may be observed. Within the newly formed hairline, no vellus hair is observed, and sometimes skin erythema is visible. In a subset of FFA patients, small reddish papules may form on the face, sometimes considered to be rough skin. bserved, which is accompanied by scalp scaling. The lesions often occur in the parietal and vertex area. A frequent accompanying symptom is itching and tenderness of the affected scalp. These conditions are sometimes worsened by sweating, exposure to sun, irritation and stress. When inflammatory symptoms subside, focal or diffuse alopecia may be observed, which gives an image of confluent white dots or milky-red areas.
bserved, which is accompanied by scalp scaling. The lesions often occur in the parietal and vertex area. A frequent accompanying symptom is itching and tenderness of the affected scalp. These conditions are sometimes worsened by sweating, exposure to sun, irritation and stress. When inflammatory symptoms subside, focal or diffuse alopecia may be observed, which gives an image of confluent white dots or milky-red areas.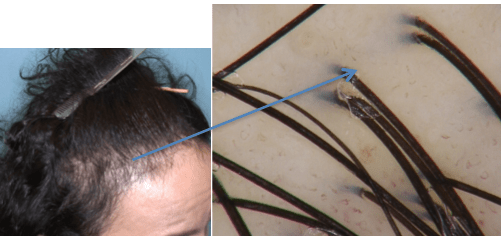 influence is connected to the reduction of estradiol and tyroxine levels in the postpartum period. The influence of these hormones o
influence is connected to the reduction of estradiol and tyroxine levels in the postpartum period. The influence of these hormones o- Telogen effluvium: Telogen effluvium (TE), first described in 1961 by Klingman, in fact encompasses a wide spectrum of clinical situations where a generalized hair loss in the telogen (rest) phase is observed. Acute and chronic telogen effluvium (CTE) have been identified.
Symptoms: In case of acute telogen effluvium, hair loss is observed on all of the scalp, although patients mostly notice balding in the frontal area. The disease starts abruptly. Telogen effluvium may be triggered by an intrinsic or extrinsic factor, which causes a vast number of hair to enter the telogen phase. The aforementioned TE-inducing factors include: diseases with high fever, surgical treatments, psychological stress, pregnancy, thyroid function disorders, end of estrogen therapy, unbalanced low-calorie diets (strict diets), iron deficiency, drugs (beta blockers, anticoagulants, retinoids, carbamazepine, vaccines), scalp diseases (psoriasis, seborrheic dermatitis of the scalp) and exposure to ultraviolet light. Telogen effluvium may be chronic and is considered to be a separate disease entity. A chronic TE may be primary or occur as a secondary condition, accompanying such general disorders as malnutrition, renal or liver failure, systemic lupus erythematosus or HIV infection. Clinically, chronic TE is manifested by a diffuse telogen hair loss afflicting the entire scalp and lasting longer than 6-8 months.
is considered to be a separate disease entity. A chronic TE may be primary or occur as a secondary condition, accompanying such general disorders as malnutrition, renal or liver failure, systemic lupus erythematosus or HIV infection. Clinically, chronic TE is manifested by a diffuse telogen hair loss afflicting the entire scalp and lasting longer than 6-8 months.
Course of disease: In case of a cute telogen effluvium, a sudden diffuse, and sometimes massive hair loss, is observed, followed by spontaneous hair regrowth within 4 to 6 months. In many cases, the improvement is spontaneous. No complete hair loss is observed. In case of chronic telogen effluvium, hair loss persists for more than 6-8 months. In anamnesis, patients often mention many years of losing hair with periods of increased intensity and remissions. Sometimes hair loss is accompanied by thinning of hair shafts, affecting all areas of the head and subjective symptoms, like hypersensitivity or tenderness of scalp. No complete baldness is observed in CTE.
Diagnosis: The diagnosis is based on a detailed medical history and analysis of the clinical picture. Apart from a trichoscopy evaluation, a trichogram is helpful.
Treatment: TE therapy is aimed at the elimination of triggering factors: endocrinopathy, metabolic disorders, deficiencies and TE-inducing drugs. Corticosteroids are used externally in TE treatment. Other medical options exist; consult your doctor to learn more. - Anagen effluvium: Anagen effluvium (AE) encompasses conditions related to diffuse loss of hair in an active growth phase, or anagen. This group of conditions includes hair loss caused by cytotoxic factors (most often cytostatic drugs, irradiation therapy, chemical toxic factors), loose anagen hair syndrome and short anagen syndrome. Some authors include in this spectrum the so-called alopecia areata incognita.
Symptoms: In case of chemotherapy-induced alopecia, a sudden diffuse loss of hair is usually observed 1-3 weeks after the first drug administration. The average incidence of hair loss is observed in approximately 65% of patients treated with cytostatic drugs and is often less intense in the case of monotherapy than in the case of therapy combining two or three drugs. Anagen effluvium of a less intense course is observed in case of patients taking drugs with a less drastic influence on the hair growth cycle (including retinoids, fluoxetine, carbamazepine). Anagen effluvium related to incorrect “anchoring” of anagen hair (the so-called loose anagen syndrome) results in hair which gives the impression of hair “that does not grow.” This syndrome mostly affects young girls (aged from 1 to 6). The similar complaints and clinical picture is observed in persons with short anagen syndrome.
 Course of disease: In cases of AE related to exposure to chemotherapeutic agents, to other drugs or toxic factors, hair regrowth may be expected once the exposure to the damaging factor ceases. Regrowing hair may be different from the previous hair; it often differs in its tendency to curl, it may also have a slightly different color.
Course of disease: In cases of AE related to exposure to chemotherapeutic agents, to other drugs or toxic factors, hair regrowth may be expected once the exposure to the damaging factor ceases. Regrowing hair may be different from the previous hair; it often differs in its tendency to curl, it may also have a slightly different color.
Diagnosis: Anagen effluvium related to cytostatic drugs is easy to diagnose, as the patients report that they are under cytostatic drug / anti-cancer treatment. Trichoscopy is very helpful in the case of differentiating other, aforementioned conditions.
Treatment: In case of hair loss caused by toxic agents, the damaging factors should eliminated if possible. There are attempts to prevent anagen effluvium related to chemotherapeutic drugs by applying scalp-cooling systems, which reduces the exposure of hair follicles to cytostatic drugs. Other medical options exist; consult your doctor to learn more.
 is considered to be a separate disease entity. A chronic TE may be primary or occur as a secondary condition, accompanying such general disorders as malnutrition, renal or liver failure, systemic lupus erythematosus or HIV infection. Clinically, chronic TE is manifested by a diffuse telogen hair loss afflicting the entire scalp and lasting longer than 6-8 months.
is considered to be a separate disease entity. A chronic TE may be primary or occur as a secondary condition, accompanying such general disorders as malnutrition, renal or liver failure, systemic lupus erythematosus or HIV infection. Clinically, chronic TE is manifested by a diffuse telogen hair loss afflicting the entire scalp and lasting longer than 6-8 months.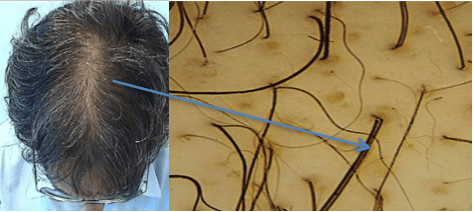 Course of disease: In cases of AE related to exposure to chemotherapeutic agents, to other drugs or toxic factors, hair regrowth may be expected once the exposure to the damaging factor ceases. Regrowing hair may be different from the previous hair; it often differs in its tendency to curl, it may also have a slightly different color.
Course of disease: In cases of AE related to exposure to chemotherapeutic agents, to other drugs or toxic factors, hair regrowth may be expected once the exposure to the damaging factor ceases. Regrowing hair may be different from the previous hair; it often differs in its tendency to curl, it may also have a slightly different color.- Medical treatment of hair loss in men: Propecia & Rogaine: The oral medication Propecia (finasteride) and the topical medication Rogaine (minoxidil) — are approved by the FDA for the treatment of common baldness (androgenetic alopecia). Minoxidil is FDA approved for men and women. Propecia (finasteride), which inhibits dyhydrotestosterone(DHT), is particularly helpful in reversing genetic baldness in its early stages. Finasteride still requires a prescription, but is available in the less expensive 5mg generic form — which can be divided into smaller 1.25mg doses using a pill cutter — and in a generic 1mg dose.
Rogaine (minoxidil) directly stimulates hair growth, but is significantly less effective than finasteride when used alone. The best results are noted when it is used in conjunction with Propecia. Minoxidil is generic and no longer requires a doctor’s prescription. Propecia is significantly more effective than Rogaine in treating hair loss, but they have additive effects when used in conjunction with one another. When both are used, over 1/3 of patients can expect visible amounts of hair regrowth. In over 90% of patients, these medications can significantly slow down further hair loss.
Use in the Crown: Since both finasteride and minoxidil were approved by the FDA for use in the crown (the back of the scalp), there is a common misconception that these drugs only work in this area. The fact is that both Rogaine and Propecia work in the front and top parts of the scalp. This makes sense, since the process of hair loss is the same in both locations. Both medications thicken fine, miniaturized hair, but both are unable to grow hair in areas that are completely bald. Since the crown usually has hair in the thinning phase for longer periods of time than the front part of the scalp, there is often a longer window of time for the medications to be useful in re-growing hair in this location. This helps to explain the relatively better response to medication in the back part of the scalp (the crown) compared to the front. That said, for prevention of further hair loss, the medications are equally important in all parts of the scalp, front and back.
Continued Use: Medications take time to work and it usually takes six months to a year to see the results. In the first few months they may cause shedding, so one needs to be patient and continue to use the medication. The effects will wear off if the drugs are discontinued and the patient will soon revert to the degree of hair loss they would have had if they had not used the medications at all.
Medicine vs. Surgery: Medications can be used alone, or can be used as part of a hair loss treatment plan that includes hair transplantation. Medical therapy works well in conjunction with hair transplantation surgery since they serve different purposes; the medical treatments work best to prevent further hair loss, whereas surgery is used to regain hair once it has been lost (or when the process is more advanced.) Unlike medication, a hair transplant does not prevent the progression of the balding process, but it is the only hair loss treatment that can restore hair permanently to a completely bald area.